Dooley Noted: 2/7/2014
The entire universe seems to know some anatomy when it comes to the rotator cuff. But how well do you know how it plays a part in the big picture?
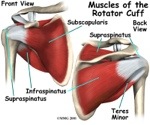
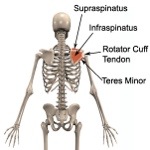
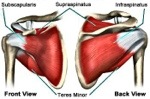
The rotator cuff muscles:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
These four muscles prevent anterior and inferior dislocation of the humerus, relative to the scapula’s glenoid fossa. In simpler terms, they help keep the shoulder stabilized.
These muscles are not the only rotators of the shoulder. They aren’t even aimed to be prime movers. They are largely stabilizing for bigger movers, like the deltoid, pectorals, and latissimus dorsi.
So, emphasis must be placed on the word “cuff,” not “rotator.”
All rotator cuff muscles are innervated by C5-C6 spinal nerves.
Four muscles, with four nerves, all from the same spinal level! This is no accident. And this area just so happens to be a common location for disc herniation in the neck.
In cases of rotator cuff tendinitis, one must always – without fail – assess movement of the neck and upper midback.
The mid to lower neck craves stability, not excessive movement. Yet people often overly use these segments and lock down the junction of the neck and midback.
If these spinal areas lock, the shoulder starts trying to take over for spinal movement.
This is why your cuff problem is not just a shoulder problem. It’s also a neck and midback problem.
The shoulder also moves in gait with the opposite hip. So, now your cuff problem is a neck, midback, and hip problem.
But, the shoulder also needs a stable platform upon which to move. So, now your cuff problem is a neck, midback, hip, and core stability problem.
Don’t get me started on the knee, ankle, and foot, which are also linked to shoulder issues.
Mix in visceral and systemic issues, and your cuff problem is officially a whole body problem.
Don’t stress! There’s hope.
Get assessed.
Practitioners: Keep one eye on the shoulder while the other is assessing the system.
Clients: If you’re getting treated for rotator cuff and the treatment only involves the shoulder, feel free to use this post to demand more solid assessment.
As always, it’s your call.
– Dr. Kathy Dooley