
Dooley Noted: 1/15/2015
The sternocleidomastoid (SCM) is an amazingly powerful muscle.
This muscle has attachments on the sternum in midline, as well as the medial one-third of the clavicle (collarbone).
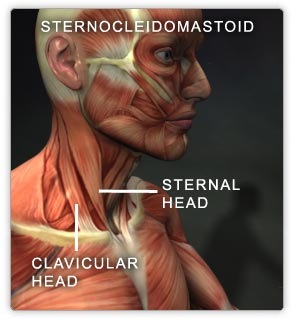
The SCM has a vast skull attachment, anchoring itself to the mastoid and superior nuchal line of the occipital bone.

Like the trapezius, the SCM is innervated by cervical ventral rami masquerading as cranial nerve XI (spinal part of accessory nerve).

So, the upper neck innervation and positioning is crucial to proper SCM function.
Because of its obliquity, the SCM has interesting and complicated functioning.
The SCM laterally flexes the neck and rotates the head to the opposite side.
The SCM can flex the cervical spine, yet extend the head.
And since it attaches to the sternum, it helps you breathe vertically.
If the sternoclavicular (SC) saddle joint is jammed, SCM is a common culprit. This can prevent full overhead movement, leading to shoulder immobility and limited upper thoracic extension.
If you see someone jutting the chin forward, suspect a facilitated SCM.
If you see neck flexion that pitches forward and can’t reach the sternum, again suspect a facilitated SCM.
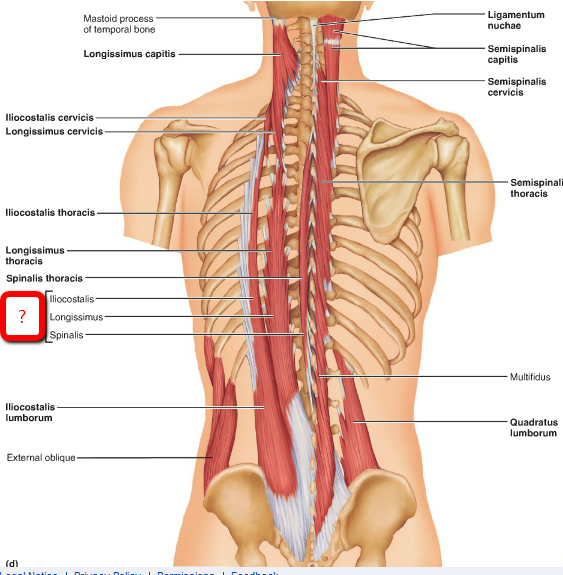
One ends up with overworked SCMs and inhibited deep stabilizing neck muscles, like longus colli and capitis.
If you see vertical chest breathing instead of a 360 chest expansion, suspect a facilitated SCM.
One ends up with inhibited torso rotators, like obliques and multifidii.
If you wake up with torticollis (wry neck), suspect a facilitated SCM.
One ends up with inferior spinal rotational inhibition.
If someone turns only the head instead of the torso and pelvis with it, suspect a facilitated SCM.
Again, look at the torso and lumbopelvic rotators to be inhibited.
You earned a cervical lordosis. Work to maintain it. Don’t let SCM inhibit your spinal stability.
As always, it’s your call.
– Dr. Kathy Dooley
