
Dooley Noted: 6/23/15
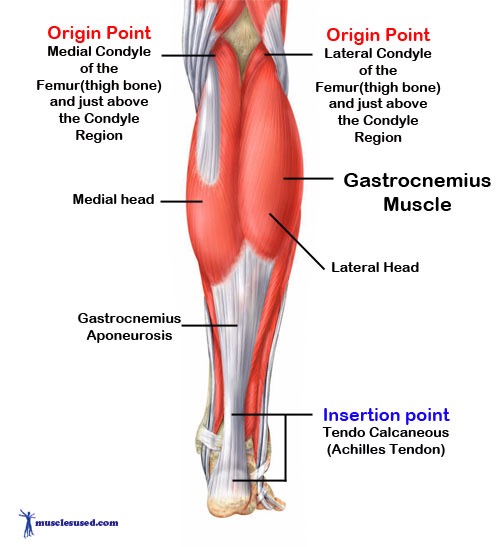
The gastrocnemius is a two-bellied, powerful muscle that forms 2/3 of the triceps surae, along with the soleus.
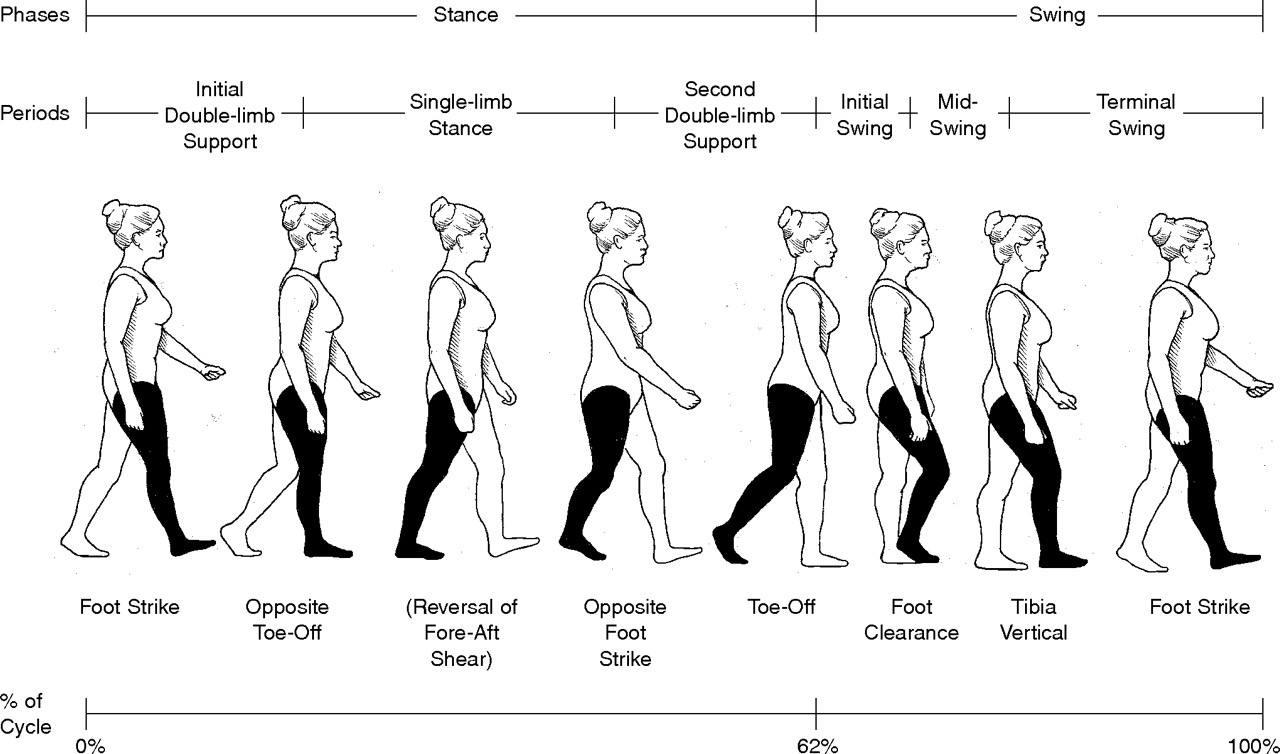
The triceps surae form the most powerful plantar flexors of the ankle, allowing one to propel forward off the back foot during gait, sprinting, jumping, and other propulsive activities.
The gastrocnemius is the multi-joint muscle of the triceps surae, moving both the talocrural (upper ankle) joint and the knee. The two heads of the gastrocnemius attach to the femoral condyles, helping to flex the knee along with muscles, like the hamstrings and popliteus.
The gastrocnemius inserts on to the middle aspect of the posterior calcaneus, or heel. Since it works in forceful propulsion, it works less to stabilize the subtalar joint (like soleus).
Thus, gastrocnemius is less important for standing balance and more for force production.
This fact makes gastrocnemius a powerful compensator when posterior chain musculature is less recruited. With their proximity to the ground, the gastrocnemius muscles quickly take over, keeping one upright and placing force into the anterior foot.
Tight gastrocnemius muscles, or “tight calves,” can result in plantar fasciitis, as the plantar fascia never gets an opportunity to return to more stretched position that is normal in pronation. In fact, most people with tight calves have difficulty in pronation, created an issue accessing an entire phase of gait.
If your calves are constantly tight, suspect that the gluteal muscles may be not as active. The glutes are stretched in pronation, so pronation may be prevented by concentrically loaded (tight and short) gastrocnemius muscles. This results in never pulling the gluteals in a healthy stretch position, so they stay in a flaccid state.
I liken it to pulling back a rubber band before firing it across the room. How can one fire something that hasn’t been loaded first?
Thus, people with tight gastrocnemius muscles end up with plantar fasciitis when they attempt to pronate. This starts a vicious cycle of attempting to keep the gastrocnemius short by wearing heels. This ultimately makes the dysfunction worse.

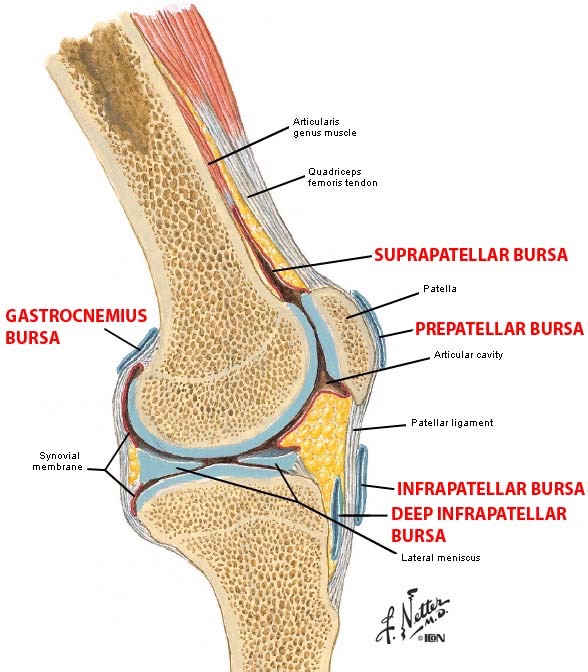
Also, facilitated gastrocnemius muscles create problems with fluid accumulation at the back of the knee.
The gastrocnemius bursa separate the heads of the gastrocnemius from the femoral condyles. The medial bursa is the most prominent, since the medial head of the gastrocnemius is typically larger. This bursa is often continuous with the knee joint capsule.
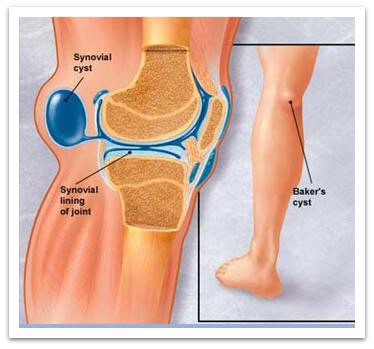
Overuse of the gastrocnemius muscles can pull fluid into the posterior knee, creating synovial cysts (i.e., Baker’s cyst). This will limit knee flexion, which is a blessing in disguise. The body is making a natural attempt at limiting the overuse of the gastrocnemius and other knee flexors, to prevent bone erosion or local tissue damage.
And the pain from bursitis can be quite fierce. This pain is also an attempt to limit the overuse of the gastrocnemius.
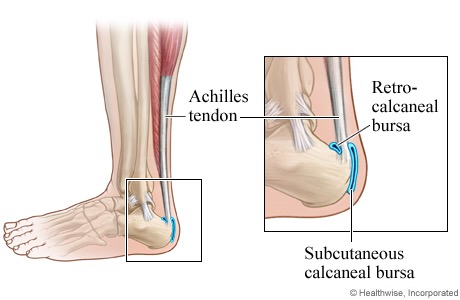
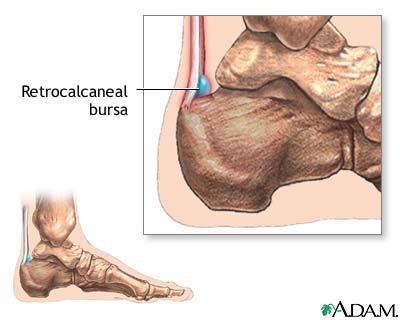
The retrocalcaneal bursa and subcutaneous bursa at the Achilles’ tendon can also be pain generators, as the calcaneus is never allowed to achieve the pronation phase of gait (dorsiflexion with eversion). The bursae get pinched and irritated, creating discomfort.
More devastating events may occur with the overuse of the gastrocnemius in a tight and short position, especially if the stubbornly tight gastrocnemius and Achilles’ tendon are suddenly asked to elongate. Tendons don’t elongate well, and the tendon can rupture right from the calcaneus.
If you lack dorsiflexion or have limited knee flexion with fluid collection, please consider the gastrocnemius muscles being overused in the kinetic chain. Look above and below this muscle to assess what may be missing.
As always, it’s your call.
– Dr. Kathy Dooley