Dooley Noted: 8/8/2015

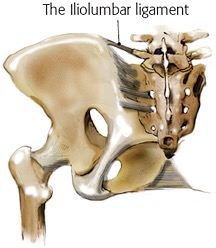
The iliolumbar ligament is a very deep, important ligament which is famous for being the inferior attachment of quadratus lumborum (QL) and the superior attachment of iliacus.

But why is that connection crucial?
This ligament is attached to many more important structures, and its anatomy must be appreciated.
The iliolumbar ligament gets its name from its connections to the L4 and L5 transverse processes medially and its lateral attachments to the iliac fossa and crest, as well as the sacrum.

In dissection, it is nearly impossible to see from the posterior, since it is buried beneath skin, superficial fatty fascia, deep muscular fascia, thoracolumbar aponeurosis, and several inches thick of erector spinae musculature.
In the anterior abdomen, it is found at the most posterior aspect, making it a major component of the posterior abdominal wall (retroperitoneum).
After removing about 30 feet of intestines and peritoneum, the structure is widely visible and seen connecting to its bony landmarks and adjacent soft tissue structures.
It is the anterior connections that make the iliolumbar ligament so significant in the building of proper intra-abdominal pressure (IAP).
The superior band of the ligament is anchored to the anterior layer of thoracolumbar fascia (a-TLF), Therefore, the iliolumbar ligament helps transmit forces build by intrinsic core muscles connecting to this a-TLF, such as the following muscles: multifidii lumborum, lumbar erector spinae, transversus abdominis, and internal abdominal oblique.
What does all that mean?
That means the iliolumbar ligament can store that kinetic energy properly built by intrinsic core on IAP and shift it to the structures to which it attaches, like QL and iliacus.
This helps explain why the loss of IAP built by intrinsics can result in improper force kinetic distribution to support the low back via QL, and the hip via iliacus.
This connection between intrinsic and extrinsic core/hip muscles helps with the transition from trunk stability to hip mobility, as well as the compression phase of gait that involves hip hiking (via QL) and hip flexion (via iliacus).
To blow your mind more, the iliolumbar ligament is actually a muscle up to the fifth decade of life!
The iliolumbar ligament receives blood and nerve supply from the lumbosacral trunk and internal iliac arteries, making this structure a vital transition area from IAP to ambulation.
This ligament often has the ilioinguinal and lateral femoral cutaneous nerves on its surface, which may result in pain referral patterns reaching the lateral thigh or into the groin.

This structure is shown in literature to have both nocioception and proprioception, enabling it to both hinder ambulation and pressure-building as well as support proper positioning for ambulation and the aforementioned force transfers.
If the QL and/or iliacus are chronically tight, consider the connection of their shared ligament and the intrinsic core via a-TLF.
You may be losing IAP, resulting in QL and iliacus stabilizing you instead of mobilizing you.
In other words, don’t skip your intrinsic core assessment (see muscles above) when someone has chronic QL and iliacus issues.
As always, it’s your call.
– Dr. Kathy Dooley