
Dooley Noted: 11/30/2015

The pudendal nerve is a somatic peripheral nerve carrying both sensory and motor fibers to an array of structures.
Since the word “pudendal” means “to be ashamed,” the structures supplied by this nerve are things one finds covered by their underwear.
The muscular structures include portions of the pelvic floor, the external anal and urethral sphincters, and perineal muscles.
The sensory structures include the vaginal and anal canals, as well as the skin of the perineum, posterior scrotum/labia, and dorsal surfaces of genitalia.
The pudendal nerve is supplied by ventral rami from S2-S4. Thus, sacral positioning and sacral foraminal occlusion may affect the pathway of this nerve.
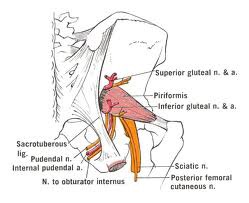
The pudendal nerve covers a treacherous path, from the inside of the true pelvis out into the gluteal areas via the greater sciatic foramen. On its pathway out of the true pelvis, the nerve is wedged between two pelvic floor supporters: the piriformis and coccygeus muscles.
Piriformis is a hip and trunk flexor, as well as an external rotator of the hip. Thus, these actions must be assessed with patients with pudendal neuropathy.
Another hip external rotator, obturator internus, creates a few important fascial connections to the pudendal nerve pathway.
Obturator internus fascia creates the lateral wall of the pudendal canal. This canal allows the passage of the pudendal neurovascular bundle from the lesser sciatic notch to their forward movement from the ischioanal fascia to the perineal spaces.

This fascia provides a lateral attachment for puboccocygeus and iliococcygeus, two anterior pelvic floor muscles partially innervated by the pelvic floor.
Thus, this fascia and these muscles affect the pudendal nerve pathway, and vice versa.

Some symptoms of pudendal neuropathy may include any of the following:
– numbness/tingling (N/T) or heightened sensation in the pudendal nerve pathway (including the external anal sphincter, perineum, posterior scrotum/labia, and dorsum of the penis/clitoris)
– pain or N/T exacerbated by hip external rotation/internal rotation, bearing down, masturbating and/or ejaculating, sexual movements, or urinating
**** Note: Pudendal nerve sends a branch to the urethral bulb, thus symptoms can increase upon urination.
Pudendal neuropathy symptoms may also be mistaken as sciatica, since the pudendal nerve often has connections to the posterior femoral cutaneous nerve. It can be mistaken for sciatica. If the discomfort also covers the pudendal nerve pathway, consider entrapment near the ischial tuberosity where the two nerves connect.
If you are having trouble with the pudendal nerve, pelvic floor and other movement therapies can be very effective in helping symptom management.
Some even consider surgery or pudendal nerve blocks, which may not get to the root cause of pudendal neuropathy.

Consider co-caring with a movement specialist that is versed in pudendal neuropathy.
As always, it’s your call.
– Dr. Kathy Dooley