
Dooley Noted: 1/13/2016
The hypoglossal nerve is the 12th cranial nerve, a nerve intimately connected with the first cervical nerve.
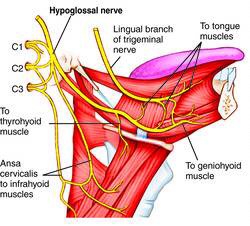
The hypoglossal nerve controls the majority of musculature to the tongue, with the exception of palatoglossus (a muscle that is vagus nerve innervated).

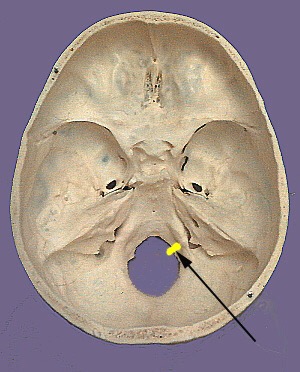
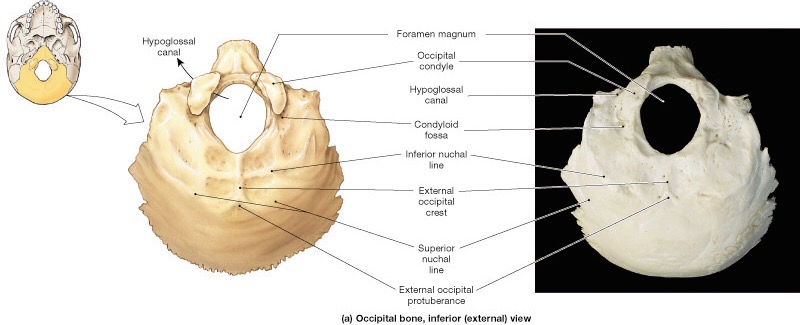
The hypoglossal nerve exits the skull via the hypoglossal canal, a canal located within the occipital condyle. Thus, the nerve function is directly affected by atlantooccipital joint movement. This is the movement of the skull relative to the cervical spine, a condylar (biaxial) joint that provides the “yes” motion of the head.
The hypoglossal nerve picks up hitchhiking C1 nerve fibers for hyoid control, such as descends hypoglossi and thyrohyoid nerve. Thus, tongue position is imperative for feedback to hyoid position for speech articulation, swallowing, and stabilizing the airway for breathing.
The hypoglossal nerve also picks up C1 nerve fibers to geniohyoid, further linking the tongue to jaw movement.
Tongue control is an activity crucial to the proper movement of the palate, pharynx, jaw and hyoid. The tongue is also a slave to the position of these structures, along with skull placement due to the styloglossus attachment to the hyoid.
Here are three very important tongue muscles and their bony attachments:
Styloglossus: styloid process, temporal bone
Hyoglossus: hyoid bone
Genioglossus: superior genial tubercle, mandible
We can assess tongue position and its carryover into distal functions by checking particular functions:
1. Tongue protrusion
2. Tongue elevation
3. Tongue deviation and rolling (side to side movement)
In a rested position for optimal breathing, the tongue must flatten across its body and meet the hard palate (roof of the mouth). The tip of the tongue should rest and gently press against the back of the incisors.
This position pulls the epiglottis forward, allowing full access to the laryngeal inlet (airway opening). Thus, optimal intrinsic core stability for inhalation can only be obtained with proper tongue positioning.
If the jaw is overly clenched or facilitated in deviation, this immediately alters tongue position. This can encourage the jaw to overact for intrinsic muscles, since the tongue can’t be properly positioned at the hard palate.
Because the hypoglossal nerve innervates these tongue muscles, cervical positioning in stability is crucial. If the atlanto-occipital joint is compressed, the hypoglossal nerve may be down-regulated on its path out the occipital condyle, creating a diminished motor output to tongue muscles.
Things to check if the tongue cannot bilaterally elevate, protrude, roll and deviate:
1. Atlanto-occipital joint compression on same side
2. Jaw deviation on same or opposite side
3. Trouble swallowing
4. Trouble with abdominal intrinsic muscle filling on same side
If abdominal stability is difficult to maintain, tongue position may be impeding it. Start assessing intrinsic abdominal muscles in inhalation, since the tongue is linked to intrinsic core stability.
If upper cervical compression is in the history, definitely assess the tongue positions.
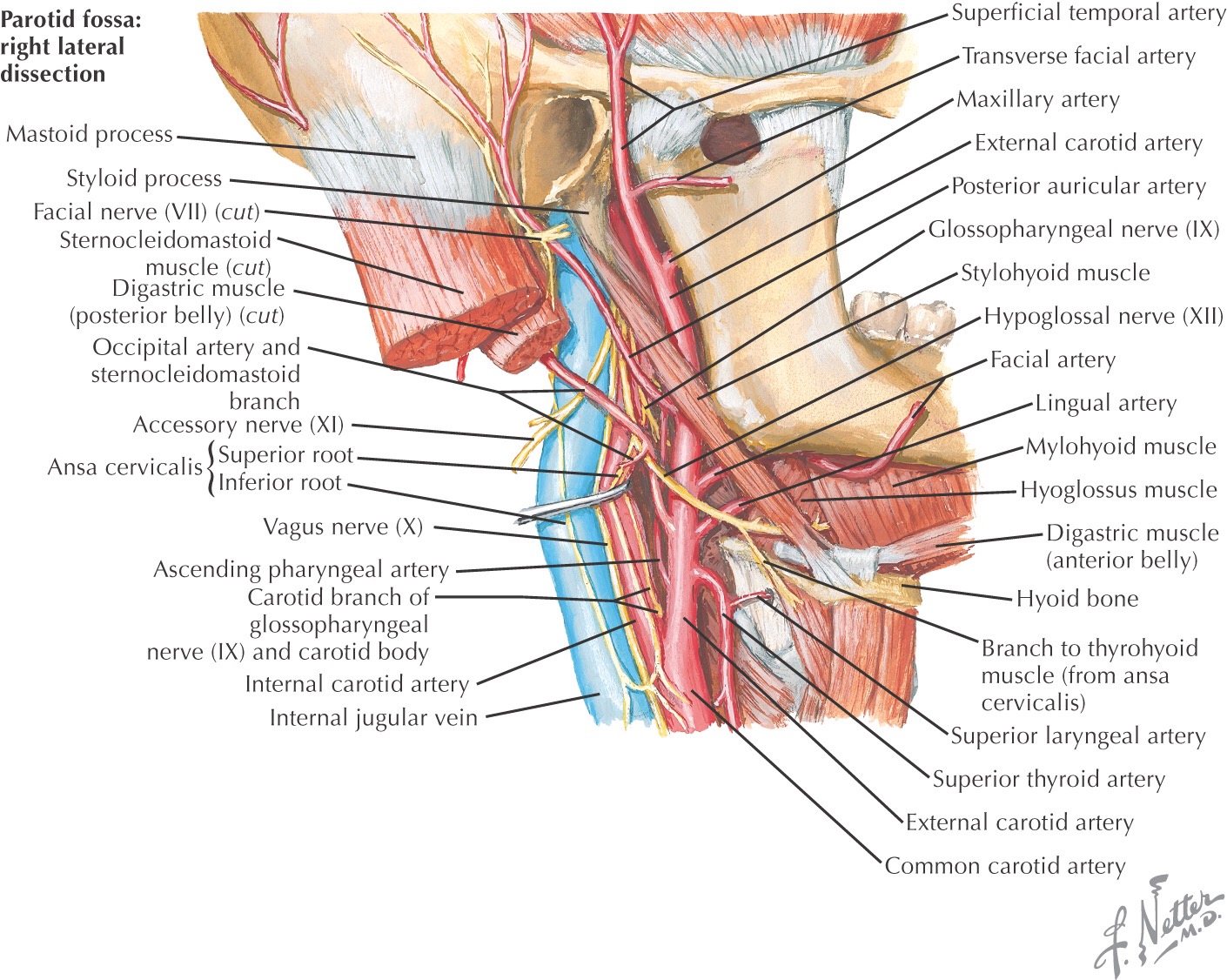
And if jaw work is not cleaning up intrinsic stability loss, definitely assess tongue position. The hypoglossal nerve runs in two anterior neck triangles, where it is susceptible to impingement by the SCM and mylohyoid muscles. (see photo)
When assigning releases of tight tongue positions, have them move opposite the action that is facilitated. In order to do this, one may need to use a tongue depressor or Q-tip to stimulate the parts of the tongue you are encouraging to stimulate.
In children, the parent may have to encourage the child to mimic the movement you’d like to encourage.
Assess the tongue and its efferent supply from hypoglossal nerve. You may be surprised at how much tongue function affects the ability to get more air on an inhale.
As always, it’s your call.
– Dr. Kathy Dooley