
Dooley Noted: 2/7/2016
Recently in lab, we performed head reflections that exposed the posterior pharynx (aka throat).
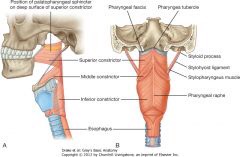
This fascinating dissection is the only time the students get to experience this view, since this is not a surgical procedure and not a common imaging procedure.
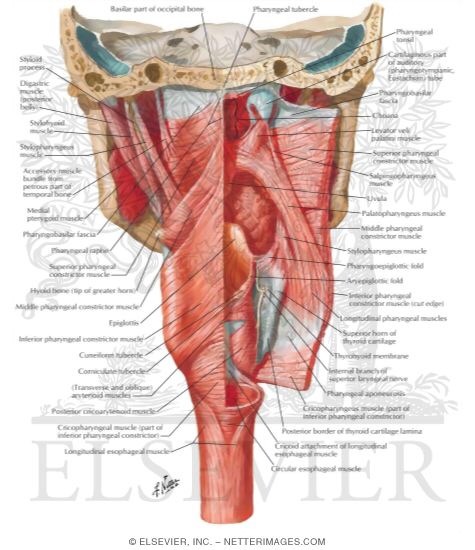
In order to complete the dissection, we have to cut through the occipital bone’s foramen magnum and disarticulate the skull from the first cervical vertebrae.
When doing this, I noticed difficulty removing the Longus Capitis muscle from the back of the pharynx.
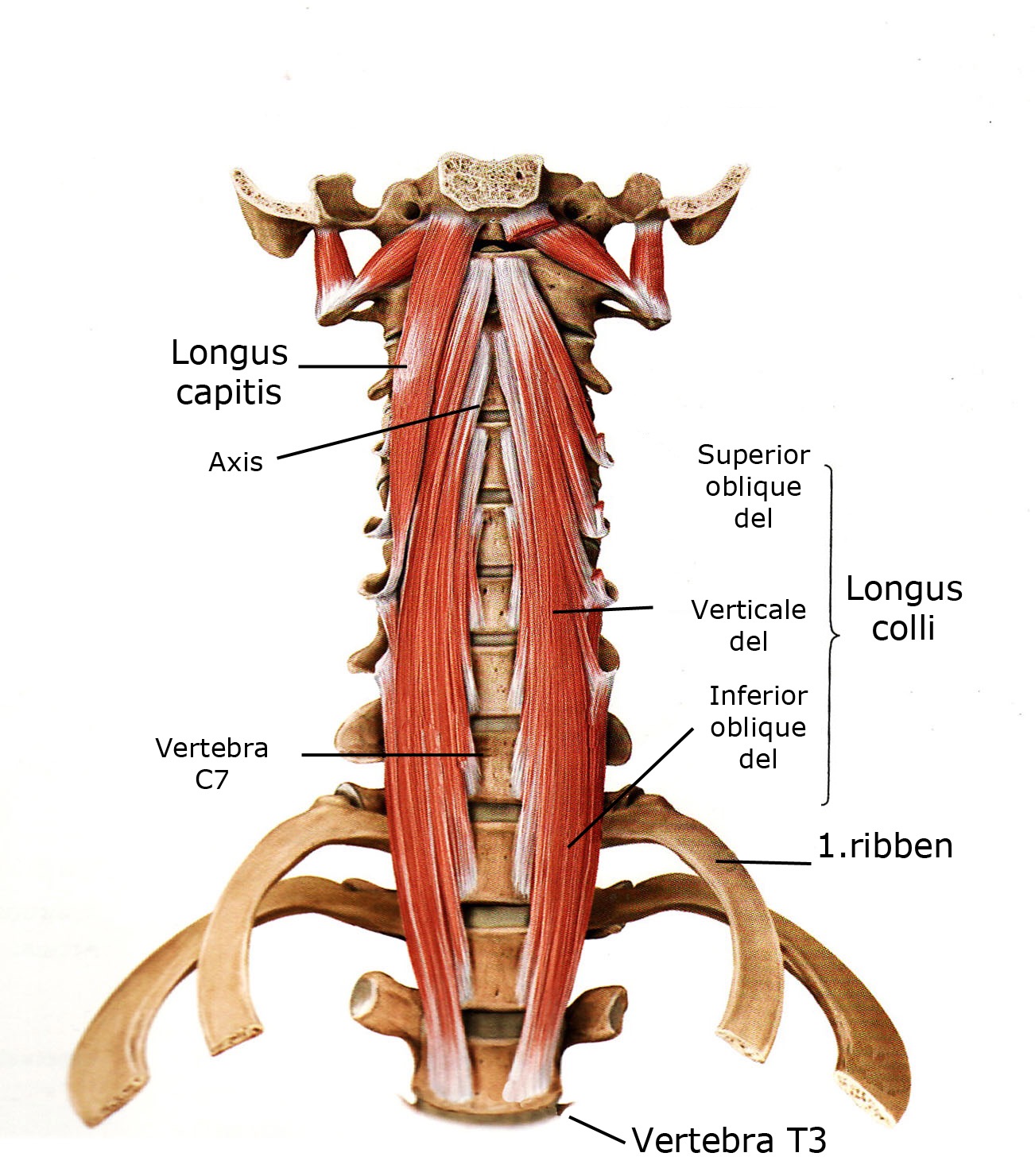
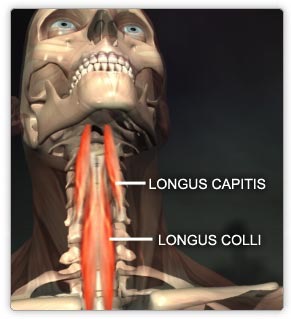
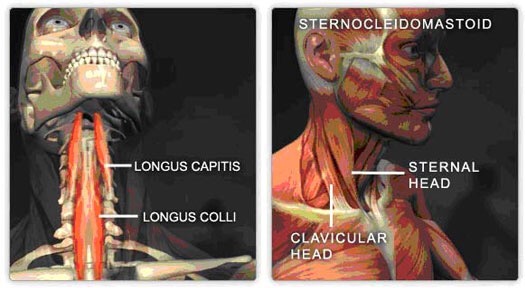
Longus Capitis is a deep cervical and head flexor, attaching from the foramen magnum to the cervical vertebrae on its anterior and lateral surfaces.
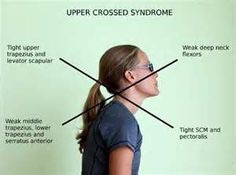
 Longus Capitis is often overridden by improper posturing in the adult, marked by anterior head carriage with excessive head extension.
Longus Capitis is often overridden by improper posturing in the adult, marked by anterior head carriage with excessive head extension.
This throws the cervical spine forward to the natural center of mass, creating cervical spinal instability and contributing to unopposed neck and extension loading.
These clients often have a head that’s perceived by the body as weighing more than when in normal position, since the forward pitching and countering by cervical extensors results in improper spinal loading patterns.
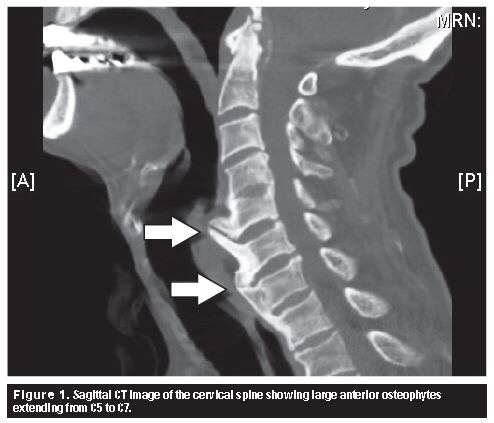
This can result in anterior vertebral osteophytosis (bone spurs) and discs that bulge anteriorly. These are attempts to create more surface area on the anterior surface, when clearly the neck biomechanics need to be improved.
Longus Capitis is often overpowered by the Sternocleidomastoid (SCM), a synergist of neck flexion but antagonist of head flexion. SCM causes the head to go into extension, thus, down-regulating Longus Capitis action at the head.
Not only do these clients tend to pitch the head forward, but they are often seen with a head jut (visible at the chin) into head extension.
They often have the inability to reach the head into flexion to the sternum.
As they tend to pitch weight forward, they may grip the ground with the toes, making the calves difficult to stretch.
Restoration of Longus Capitis can improve anterior and lateral cervical spinal stability to prevent disc herniations and osteophytosis of the cervical spine.
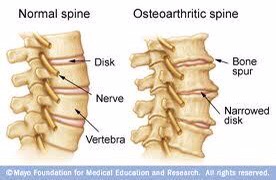
Bone spurring is a particular concern for those with long-standing cervical stability loss in flexion, since the spurs create difficulty in swallowing.
Ease in swallowing can be improved by improving head and cervical spinal movement into flexion.
Prevent disc bulges and bone spurring by improving the function of Longus Capitis.
As always, it’s your call.
– Dr. Kathy Dooley