
Dooley Noted: 2/19/2016
Since I can’t go an hour without someone asking me about the “new quad” being identified, I took it upon myself to discuss a clinically important – yet often uncredited – bundle of slightly collagenated tissue that resembles fascia and tendinous properties.
While the migrant quad belly shows no clinical significance other than a “cool” factor, the aforementioned unnamed fascia is a connection between vastus medialis and adductor magnus that is not quite a septum but certainly could serve as one.
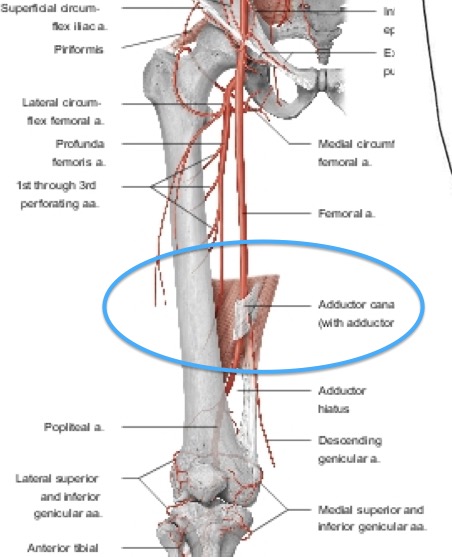
I see it in 100% of cadavers, tethering across the saphenous nerve in the adductor (subsartorial) canal. In each cadaver, I must release this thick fascia before my students can properly visualize the saphenous nerve passing through the adductor canal – but not into the adductor hiatus.
My students affectionately deemed this the “Dooley fascia,” since it isn’t clearly names and serves as an important protector and binder for the saphenous nerve.
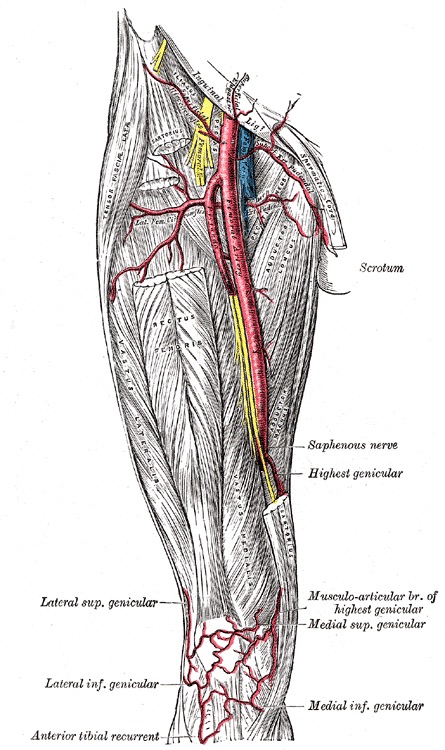
The fascia also serves as a clear impingement site for this nerve, which supplies innervation to the skin of the medial knee, medial leg, and medial foot, as distally as the first metatarsal-phalangeal joint (read: big toe knuckle).
This overlooked cause of knee pain and medial leg and foot tingling may be addressed by assessment of this fascial bind, and the muscle to which it is attached.
In an overworked adducting thigh, the vastus medialis can be pulled into a locked long position, tethering the thick fascia across the saphenous nerve.
Conversely, an overworking vastus medialis in the sagittal plane can lock the adductor in a long position, again tethering the fascia across the saphenous nerve.
This is one more reason why quad and adductor function must always be assessed with medial knee, leg and foot pain.
Since the saphenous nerve delivers the L4 dermatome from the femoral nerve, nerve root impingement at the lumbar spine must always be assessed with pain or tingling along the saphenous nerve’s distribution.

Very commonly, those with low back issues have knee issues, due to forward force bearing and irritation of these two uniplanar joint systems that have their second degree of freedom over-utilized.
After you clear the low back for involvement, consider this functional important, often ignored fascial bind across a nerve with a vast cutaneous delivery system.
As always, it’s your call.
– Dr. Kathy Dooley