
Dooley Noted: 5/27/2016
In the fitness and rehab communities, we are versed on the idea of a Joint-By-Joint Approach to clinical auditing, assessment, and screens for functional movement.
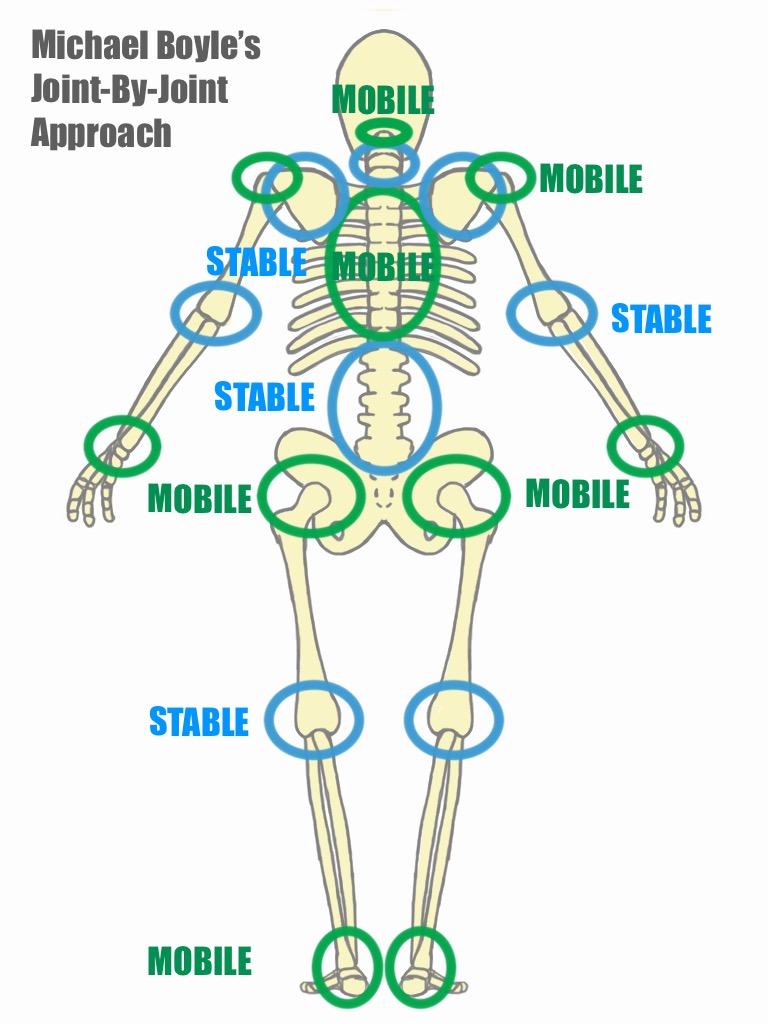
Common movement cravings per body part are easily seen in this graphic, attributed to Mike Boyle’s thought process of this approach to joint mechanics, relative to each region.
While this approach is commonplace in our fields, it’s not common knowledge to people outside of our fields.
These are the people coming to us for help.
For most of my patients, it’s news that the entire neck does not crave mobility and stability equally.
They reignite my fascination daily with their own intrigue of finding their lumbar spine pain comes from a back that already moves too much – even if it feels tight.
But as you show the joint mechanical grouping of the famous poster, you show one joint trading off its motion craving.
Then, you clearly see the spiraling events of why one’s ankle sprain from fourth grade becomes ankle immobility. That leads to knee compensatory movement for the ankle when the hinge-like knee craves more stability.
This will prevent the hip from moving in its massive ranges, since the knee is already moving faster and with more fervor.
Lock up the hip, and you start moving the uniplanar back joints for the triplanar hip.
So, you’ve bought Into the trade off.
Now what? Which part do you unravel first?
Here are some tips on knowing where to start:
1. Chief complaint: Where is the discomfort? This is likely the site of one part moving too much for something else adjacent in the kinetic chain.
2. History: Find the oldest injury, even if it’s an old sprain they barely remember. Unless property rehabilitated, the body holds onto old injuries.
3. The movement screen/assessment: start with the worst balance, range of motion, or most compensatory pairing you visualize or test.
4. If that all fails, start anywhere. Seriously. Just start. Start with the foot. Or start with breathing. At whichever end you start, you’ll end up unwinding this issues ifyou follow the rules of the Joint-By-Joint Approach.
Yes, your left neck pain is linked to your opposite knee pain.
Yes, your lumbar disc herniation may be linked to your old ankle sprain.
Yes, your hip pain is linked to a lumbar stability loss.
Please consider that your elbow, knee, or back pain may not be a problem primarily with the area that hurts.
When you are scouting a manual therapist or training coach, make sure they have these conversations about joints with you.
Look closely at that diagram, and start to understand that if you trade off now what a joint region craves, you’ll be chasing pain and dysfunction around for a while.
As always, it’s your call.
– Dr. Kathy Dooley